Head, Neck, & Jaw
Jaw and Neck Pain: TMD, Posture and What May Be Driving It
- Updated - July 17, 2026
Jaw pain does not always begin or end at the jaw. Learn how the joint, chewing habits, stress, breathing and the neck can interact, and what a thorough assessment should look for.

Jaw pain has a habit of returning. The muscles are massaged, the joint is checked or a night splint is fitted, and for a while the clicking, morning tightness or dull ache in front of the ear improves. Then the symptoms gradually return.
This does not mean the treatment was useless. It may mean that only one part of the problem was addressed. Persistent jaw pain is often influenced by several overlapping factors: the joint itself may be irritated, the chewing muscles may be overworking, and clenching, grinding, stress, sleep, breathing and the position or movement of the neck may all be contributing.
The important question runs deeper than where it hurts:
What is placing the jaw under more load than it can currently manage?
This article explains how the temporomandibular joint works, what temporomandibular disorders are, how the jaw and neck can influence one another, and what good assessment and treatment should involve.
This article provides general health information and is not a substitute for individual medical, dental or allied health advice.
What is the temporomandibular joint (TMJ)?
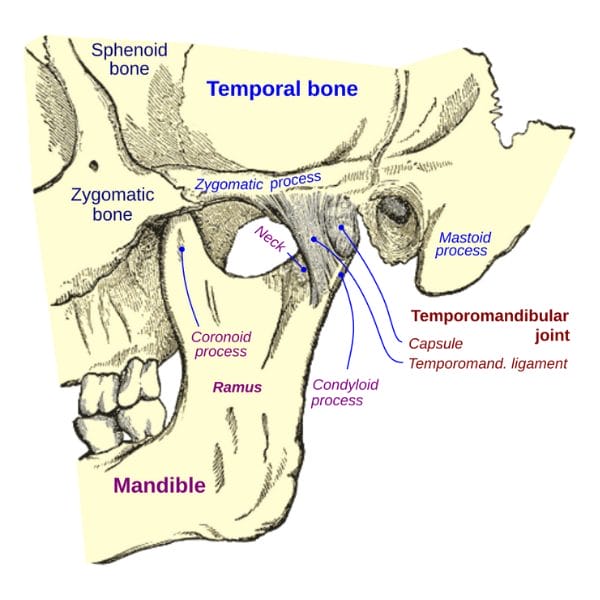
The temporomandibular joint, usually shortened to TMJ, is located just in front of each ear. It is where the lower jaw, or mandible, connects with the temporal bone of the skull.
Each joint includes:
- The rounded upper end of the mandible, known as the condyle
- A shallow socket in the temporal bone
- A flexible articular disc between the two bones
- A capsule and ligaments that help contain and support the joint
- Muscles that control jaw movement and provide stability
The disc helps the surfaces of the joint move smoothly against one another and distributes pressure during speaking, chewing and other jaw movements.
What movements does the TMJ perform?
The jaw needs to perform several different movements:
Opening and closing
Opening the mouth combines rotation of the jaw with a small forward glide of the condyle and disc.
Protrusion and retrusion
The lower jaw slides forward and then returns backwards.
Lateral excursion
The jaw moves from side to side, allowing food to be ground between the teeth.
These movements require coordination between both jaw joints, the chewing muscles, the tongue, the throat and the neck. The jaw does not operate as an isolated hinge.
What is TMD?
The TMJ is the anatomical joint. Temporomandibular disorders, or TMDs, are a group of conditions that affect the jaw joints, the chewing muscles or the surrounding tissues.
Some TMD presentations are primarily muscular. Others involve the disc or joint surfaces. Many involve more than one structure at the same time.
Common symptoms of TMD
Symptoms can include:
- Pain or tenderness in the jaw or chewing muscles
- Pain around the face, temple or in front of the ear
- Jaw stiffness or restricted opening
- Pain when chewing, speaking or yawning
- Painful clicking, popping or grating
- Jaw locking or temporarily catching
- Headaches
- Neck and shoulder discomfort
- Earache or a feeling of fullness around the ear
- Ringing in the ears
- A change in how the bite feels
- Swelling around the jaw joint
Jaw sounds are not automatically a sign that something is wrong. Clicking or popping that occurs without pain, locking or loss of movement is common, and it does not always require treatment.
Discover a practitioner near you.
Looking for a practitioner near you? Our extensive network of qualified professionals is here to help you.
What causes jaw pain and TMD?
There is rarely one explanation that applies to every person. TMD can involve the joint, the disc, the chewing muscles, previous injury, arthritis, clenching, grinding, stress and changes in how pain is processed. Sleep quality, general health and the neck may also influence how symptoms develop or persist.
A useful way to organise these contributors is to consider three areas.
- What can the jaw currently tolerate?
This is the jaw’s capacity. Arthritis, inflammation, disc problems, previous trauma or a period of painful and guarded movement can reduce the amount of load the joint and its muscles can comfortably manage. Activities that were previously harmless may then become provocative.
Capacity is not fixed. With the right management, it can often improve.
- What is the jaw being asked to do?
This is the jaw’s daily load. Common sources of additional load include:
- Clenching while concentrating
- Grinding during sleep
- Chewing predominantly on one side
- Frequent gum chewing
- Nail biting
- Holding the jaw tense while driving or working
- Repeatedly checking or forcing a clicking jaw
- Long periods of talking or chewing during a flare-up
These habits are not character flaws. Many are automatic responses to concentration, stress or discomfort, and they need to be identified before they can be changed.
- What else is influencing the jaw?
The jaw is coordinated with the neck, tongue, throat and breathing system. Its movement may also be influenced by stress, sleep, pain sensitivity and the way the head is being supported.
This does not mean that posture is the cause of every jaw problem. It means that the jaw should be assessed alongside the systems around it, rather than in isolation.
Persistent TMD commonly involves an interaction between capacity, load and the wider context in which the jaw is working. This is one reason a single treatment may produce short-term improvement without resolving the entire problem.
Is your jaw the problem or the messenger?
This is the question we ask about any persistent jaw presentation:
Is the jaw driving the problem, or is it compensating for something else?
This comes from the clinical reasoning framework we teach practitioners, the Clinical Triangle.
Driver
The structure, behaviour or process creating enough disturbance to organise the wider pattern.
The driver might be local to the jaw: an irritated joint, a significant clenching pattern, an acute injury or restricted movement after a dental procedure. In other cases, the primary driver may sit elsewhere.
Compensation
The body's response to the driver. Compensations are strategies the body uses to maintain function, avoid pain or create stability.
A chewing muscle that feels chronically tight may be overworking because of clenching, or it may be helping manage an altered jaw pathway or neck restriction. Releasing it may feel excellent, yet the result may not last if the reason it was overworking remains unchanged.
A compensating muscle often tightens again because the job it was performing is still there.
The aim here is diagnostic rather than dismissive. Instead of labelling every symptom as compensation, a good practitioner tests whether the painful area is generating the problem or responding to it.
What can the timing of symptoms tell you?
The way symptoms behave can provide clues, although timing alone cannot establish a diagnosis.
Worse on waking
Morning pain or stiffness may indicate night-time clenching or grinding. Sleep position, sleep quality and other sleep-related factors may also contribute.
Builds through the day
Symptoms that increase as the day progresses may reflect accumulated chewing, talking, daytime clenching, stress or sustained demand through the head and neck.
Provoked by chewing or opening
Pain that reliably increases with chewing, yawning or specific jaw movements raises the likelihood of a local joint or chewing-muscle component.
Changes during stressful periods
A strong relationship with stress may suggest increased clenching, muscle guarding, altered sleep or heightened nervous-system sensitivity.
Constant and unaffected by movement
Pain that is persistent, worsening and not meaningfully changed by jaw or neck movement deserves medical or dental assessment. It may not be a straightforward mechanical TMD presentation.
These patterns are clues, not conclusions. A practitioner should test the possible relationship rather than assuming that symptom timing proves the cause.
How are the neck and jaw connected?

The relationship between the cervical region and the jaw is real, though it is often oversimplified. People with TMD frequently also report neck pain or disability, and research has identified associations between jaw disability and cervical disability, reduced cervical movement, tenderness and changes in sensory-motor function.
These are associations. They do not prove that a particular posture caused the TMD, and the evidence linking a static head position directly to TMD remains mixed. The neck can influence the jaw through several overlapping pathways.
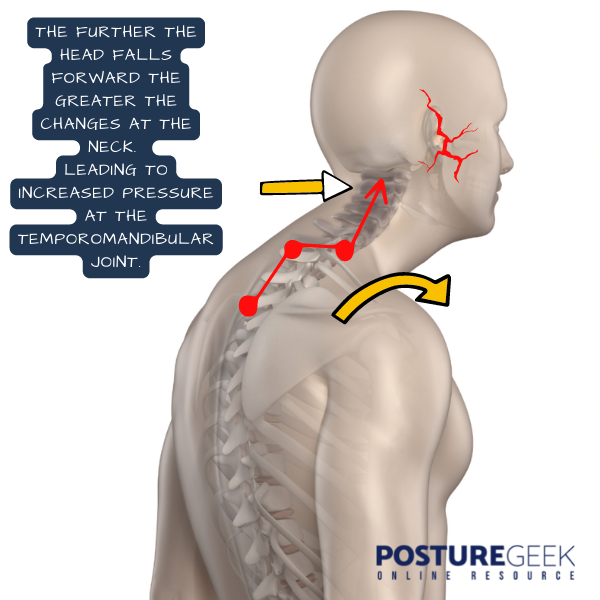
Head position can change the jaw’s starting point
The lower jaw hangs from the skull and is guided by muscles that attach around the head, face and throat. Changing the position of the head can alter the jaw’s resting relationship and its pathway during opening and closing. For some people, a sustained head position may increase the work required from the jaw and neck muscles. This is a possible contributor rather than proof of causation.
The jaw and neck must coordinate
Speaking, swallowing, chewing and breathing involve coordinated activity across the jaw, tongue, throat and upper neck. If one part of that system becomes painful, stiff or poorly coordinated, other areas may increase their activity to maintain the task.
The regions share sensory processing
Sensory information from the upper cervical region and the trigeminal system, which serves much of the jaw and face, is processed through closely related neurological pathways. This helps explain why neck problems can sometimes contribute to facial pain or headaches, and why jaw symptoms may be felt beyond the joint itself.
Breathing and resting oral posture may matter
At rest, the jaw is generally most relaxed when the teeth are slightly apart, the lips are comfortably together, the tongue rests gently against the palate without being forced, and breathing occurs comfortably through the nose. Persistent mouth breathing changes this resting arrangement and may influence tongue and jaw-muscle behaviour in some people.
Mouth breathing is not always a habit. Nasal congestion, allergy, sinus problems and airway restrictions may be involved, so persistent difficulty breathing through the nose should be assessed rather than simply corrected through effort.
A better way to think about posture
Posture is more than whether someone is sitting straight enough. There is no single perfect position that everyone should maintain throughout the day, and the body is designed to move between positions.
Problems are more likely to develop when:
- One position is sustained for long periods
- The person has limited movement options
- The position noticeably changes symptoms
- The muscles are continually working to maintain it
- The body cannot comfortably return from it
For someone with jaw pain, the useful question changes. Rather than asking whether a posture is good or bad, ask whether this position increases the load on the jaw, and whether the person can move out of it comfortably. That is something that can be tested.
Can improving neck function help TMD?
For some people, yes. Treatment directed towards the jaw, neck or both may improve pain and mouth opening, particularly when the cervical region is clearly involved. The evidence is more supportive of an individualised combination of education, exercise and appropriate hands-on treatment than of any single corrective technique.
The overall evidence remains variable, which is another reason treatment needs to be tested against the individual’s response. Practical starting points may include the following.
Notice your clenching triggers
Pay attention during computer work, driving, concentrated tasks, exercise, stressful conversations and phone use. Simply noticing that the teeth are touching can be the first useful intervention.
Lips relaxed, teeth apart, jaw unforced.
Vary your position
Rather than holding yourself rigidly upright, change position regularly, support your arms during screen work and bring frequently used screens closer to eye level when practical. The goal is more movement choice, not permanent muscular effort.
Use gentle jaw movement
During a flare-up, small and comfortable opening and side-to-side movements may help maintain mobility. Avoid forcing the mouth open, repeatedly provoking a click or stretching aggressively into pain.
Review sleep support
A pillow should support the head without forcing it sharply forwards or allowing it to fall into a prolonged side bend. There is no single correct pillow for everyone, and body size, sleeping position, mattress firmness and personal comfort all matter.
Address persistent mouth breathing
Do not force nasal breathing if the airway feels restricted. Persistent congestion, snoring, disrupted sleep or difficulty breathing through the nose may warrant assessment by a GP, dentist or relevant specialist.
Build capacity gradually
When symptoms settle, graded jaw and neck exercises may help restore movement, confidence and tolerance. The aim is to help the jaw tolerate normal activity again, rather than to protect it from all load.
What good treatment for TMD should look like

It should begin with an appropriate assessment
A good assessment may include the location and behaviour of the pain, jaw opening and closing, joint sounds, locking or deviation, chewing-muscle tenderness, neck movement and symptoms, dental history, clenching and grinding, sleep and stress, recent injury or dental procedures, breathing and resting oral posture, and relevant medical warning signs. Not every person needs every test, and the assessment should be guided by the presentation.
The practitioner should explain their reasoning
You should understand what the practitioner believes may be driving the problem and what they intend to test. A diagnosis or treatment plan should rest on clear reasoning, not on a vague statement that everything is “out of alignment.”
Your response should be rechecked
Treatment should operate like an experiment. The practitioner forms a reasonable hypothesis, applies an intervention and then reassesses the symptom or movement. If the jaw changes, the hypothesis gains support. If it does not, the practitioner should reconsider the explanation rather than repeating the same treatment more forcefully.
Local treatment can be useful
Hands-on treatment of the chewing muscles and surrounding tissues may reduce pain and guarding. Jaw exercises, education and temporary changes to food consistency may also help during a flare-up. Local treatment keeps its value even when the neck is involved. The question worth asking is whether local treatment on its own is enough.
The plan should include active management
Treatment should eventually help you understand what aggravates the symptoms, how to reduce unnecessary load, how to move the jaw comfortably, how to rebuild tolerance, and when to seek further assessment. Repeated passive treatment without a clear plan may create temporary relief but limited long-term change.
Care should be collaborative
Dentists and TMD-focused dental practitioners are important when there is tooth damage from grinding, significant dental disease, a new or changing bite, suspected joint pathology, locking or marked restriction, or a need to assess whether a splint is appropriate.
What treatments are used for TMD?
Treatment should match the presentation. Most people should begin with conservative and reversible approaches.
Self-management
This may include temporarily choosing softer foods during a flare-up, avoiding gum and very chewy foods, applying heat or cold depending on preference, reducing nail biting and unnecessary clenching, using gentle and comfortable jaw movements, and taking suitable short-term pain relief after advice from a doctor or pharmacist.
Exercise and physical treatment
Depending on the findings, treatment may include jaw mobility exercises, graded strengthening, coordination exercises, neck movement and endurance work, education about habits and loading, and manual therapy directed towards the jaw, neck or both.
Dental management
A dentist may recommend a splint in selected cases, particularly to protect the teeth from grinding damage. A splint does not necessarily stop clenching or resolve every TMD presentation, and it should be monitored, particularly if it changes the bite or increases symptoms.
Permanent changes to the bite, extensive dental procedures or orthodontic treatment should not be undertaken solely on the assumption that they will cure TMD without a clear dental indication.
Specialist treatment
Injections, more invasive procedures and surgery are generally reserved for selected cases with a clear diagnosis that have not responded to appropriate conservative care. The more irreversible the treatment, the stronger the diagnosis and justification should be.
When should jaw pain be assessed promptly?
Seek prompt medical or dental assessment if you notice:
- A jaw that locks open or closed
- A sudden or significant loss of mouth opening
- A new change in your bite
- Jaw pain after a direct injury
- Facial swelling, warmth or fever
- Numbness, weakness or altered sensation in the face
- A persistent lump in the face or neck
- Unexplained weight loss or significant systemic illness
- New one-sided hearing loss or persistent ear symptoms
- Pain that is constant, worsening and unaffected by movement
- A severe new headache, visual disturbance or jaw fatigue when chewing
Finally
Jaw pain that returns after treatment does not mean nothing can help. It may mean the jaw is only one part of the presentation. The joint, chewing muscles, daily habits, stress, sleep, breathing and cervical region can all influence how much load the jaw carries and how well it tolerates that load.
Sometimes the jaw is the driver, and sometimes it is compensating for something else. Often both local and wider factors need attention. A thorough assessment holds off on assuming that posture is the cause, while staying willing to test whether the neck and the rest of the structure are contributing.
Good care goes beyond loosening the place that hurts. It works out why the area is hurting, reduces unnecessary load, and helps the jaw return to comfortable, confident function.
References and further reading
- National Institute of Dental and Craniofacial Research. TMD (Temporomandibular Disorders). This is a genuine NIDCR/US National Institutes of Health health-information page.
- Healthdirect Australia. Temporomandibular joint dysfunction. This is a genuine Healthdirect Australia page, last reviewed in November 2025.
- Lomas J, Gurgenci T, Jackson C, Campbell D. Temporomandibular dysfunction. Australian Journal of General Practice. 2018;47(4):212–215. doi:10.31128/AFP-10-17-4375. This is a real clinical article published by the RACGP.
- de Oliveira-Souza AIS, Ferro JKO, Barros MMMB, de Oliveira DA. Cervical musculoskeletal disorders in patients with temporomandibular dysfunction: A systematic review and meta-analysis. Journal of Bodywork and Movement Therapies. 2020;24(4):84–101. doi:10.1016/j.jbmt.2020.05.001.
- Cuenca-Martínez F, Herranz-Gómez A, Madroñero-Miguel B, et al. Craniocervical and cervical spine features of patients with temporomandibular disorders: A systematic review and meta-analysis of observational studies. Journal of Clinical Medicine. 2020;9(9):2806. doi:10.3390/jcm9092806. Your version omitted “of observational studies” from the full title.
- Idáñez-Robles AM, Obrero-Gaitán E, Lomas-Vega R, Osuna-Pérez MC, Cortés-Pérez I, Zagalaz-Anula N. Exercise therapy improves pain and mouth opening in temporomandibular disorders: A systematic review with meta-analysis. Clinical Rehabilitation. 2023;37(4):443–461. doi:10.1177/02692155221133523.
- La Touche R, Martínez García S, Serrano García B, et al. Effect of manual therapy and therapeutic exercise applied to the cervical region on pain and pressure pain sensitivity in patients with temporomandibular disorders: A systematic review and meta-analysis. Pain Medicine. 2020;21(10):2373–2384. doi:10.1093/pm/pnaa021.
PLEASE NOTE
PostureGeek.com does not provide medical advice. This information is for educational purposes only and is not intended to be a substitute for professional medical attention. The information provided should not replace the advice and expertise of an accredited health care provider. Any inquiry into your care and any potential impact on your health and wellbeing should be directed to your health care provider. All information is for educational purposes only and is not intended to be a substitute for professional medical care or treatment.
About the author
Find Expert Posture Practitioner Near You
Discover our Posture Focused Practitioner Directory, tailored to connect you with local experts committed to Improving Balance, Reducing Pain, and Enhancing Mobility.